

Thank you for visiting my website. You will find information about my work and my activities as the Member of Parliament on behalf of the people of Walsall South. You can contact me directly through the website and find details about my office. Owing to Covid-19 I am unable to meet at surgeries, and I am now conducting telephone surgeries. I use the House of Commons Parliamentary answering service when my office is busy or out of hours. Please leave your message with them and remember to give your name, address and contact details. The Answering Service will send me an email with your message
If you have any problem or issue you think I may be able to help you with, please do get in touch.
Please note that Members of Parliament are not an emergency service so do contact the appropriate emergency services when required.
I would like to thank the NHS for their wonderful service during the pandemic.
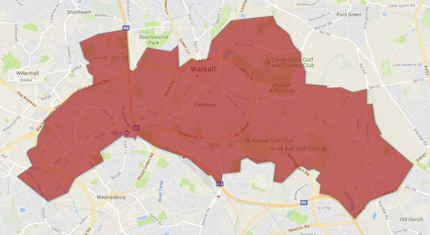
About Walsall South
Do you live in the constituency? Follow the link below to check that Valerie is your MP.


Press Releases
Keep updated with the latest news locally, media coverage and news from Parliament.

I was delighted to visit the Chelsea flower show to discuss the issues in the Agricultural Industry. The Chelsea Flower show came 5th in world to do list. it is a show of excellence and creativity and is now in its 111 year. It showcases horticultural skill and is the most sustainable green audit; water and biodiversity; garden tourist gen 3 billion ;Chelsea facilitates scientific and other work; it showcases scientific plants for purpose ;flood mitigation, pollution and greening cities; This year they are including children - the Children's Judges Panel which picked the Octavia Hill Garden; and the Garden titled no adults allowed; it teaches children about plant names and RHS supports plant a tree campaign for school gardening; pocket gardens in hospitals; future national gardens; environmental horticultural groups. there are Key industry challenges and problems.every school to grow a plant to focus on education; the planning system to look at where reservoirs are placed; Green space is important;growers, retailers and manufacturers are all working to a 20% reduction in carbon footprint Water aid garden and the use of grey water. Whilst there are many challenges in the industry these challenges and that of climate change are being met by research. the CFS hopes to be peat free by 2025. IThis garden ( right) The Octavia Hill Garden was chosen by the Children Judges Panel as the best garden . One in three people in Britain do not have access to a natural green space within 15 minutes walk from their home. Gardens of all shapes and sizes have the power to help people and nature thrive.
The Sustainable Garden is an exhibit from last year and was recycled for this Garden.
Names of the trees
No adults allowed in the garden! I received a sticker and then entered. There was a slide and a tree house.
The clematis were all grown in peat free soil and RHS Chelsea hopes to be peat free by 2025.
Mushrooms growing in the greenhouse; a display and the Asian Hornet is a concern for the industry.
The Inquiry into the Infected Blood Inquiry published its report on 20 May 2024. Chaired by Sir Brian Langstaff a former Judge of the High Court it runs to 7 volumes. This is the Summary of the report:
"Patients have received blood or blood products from the NHS since it began in 1948. Many of those treated with them, particularly between 1970 and 1998, died or suffered miserably, and many continue to suffer. This was not as a direct result of the underlying condition or illness that took them to the NHS in the first place, but as a result of the treatment itself. This would be catastrophic enough if they were the only victims. But the treatment has caused others to suffer too – partners, family, children, friends – some by being themselves infected, some by having to watch loved ones die, some by having to give their lives to caring; and almost every one of them, infected and affected, suffering in almost every aspect of their lives. I have to report a catalogue of failures which caused this to happen. Each on its own is serious. Taken together they are a calamity. Lord Winston famously called these events “the worst treatment disaster in the history of the NHS”. I have to report that it could largely, though not entirely, have been avoided. And I have to report that it should have been.
I have also to report systemic, collective and individual failures to deal ethically, appropriately, and quickly, with the risk of infections being transmitted in blood, with the infections when the risk materialised, and with the consequences for thousands of families.
There were around 4,000 to 6,000 people with bleeding disorders in the UK at any one time. Around 1,250 were infected with HIV. The best estimate is that this included 380 children. Almost all infected with HIV were also infected with Hepatitis C and some with Hepatitis B and Hepatitis D as well. Three quarters of these 1,250 adults and children have died. A larger number still (between 2,400 and 5,000 people with bleeding disorders) who were not infected by HIV received blood products infected with one or more hepatitis viruses, and developed chronic Hepatitis C.
People who were infected by transfusions, rather than by blood products, were infected in even greater numbers. Between 80 and 100 were infected with HIV after a blood transfusion. Approximately 26,800 were infected with Hepatitis C after a blood transfusion, often linked with childbirth or surgery, but also from transfusions to treat thalassemia, sickle disease, or leukaemia, or tissue transfer. It has not been possible to estimate the number of people infected with chronic Hepatitis B due to limited data.
A significant number of people who received blood products and some who received blood transfusions have since been told that they are at an increased risk of vCJD, and should alert their medical practitioner or dentist prior to treatment. This in turn has compromised their access to that treatment.
The scale of what happened is horrifying. The most accurate estimate is that more than 3,000 deaths are attributable to infected blood, blood products and tissue.
To understand the failings, it is necessary to set out the reasoning behind my conclusions in some detail. They need to be explained and set in context. That will follow in the chapters of this Report.
What follows makes for hard reading. For now, though, the headline points are these:
The principal infections considered by the Inquiry are Hepatitis (B and C) and HIV. The transmission of vCJD is also considered.
It was well known from at least the early 1940s, and became clear beyond doubt in the mid1940s, that blood transfusions or the use of plasma could transmit “serum hepatitis”. It was known that this could be fatal, or lead to serious long-term disease, liver failure, cirrhosis and cancer. The virus responsible for Hepatitis B was identified by the early 1970s. The virus responsible for Hepatitis C was not identified until 1988, but it was apparent at least from the mid 1970s that non-A non-B Hepatitis (as it was known prior to 1988) was responsible for the majority of post-transfusion hepatitis cases and that just as Hepatitis B could have serious long-term consequences, so too might non-A non-B Hepatitis.
Awareness of AIDS began in 1981, and it was apparent by mid 1982 that whatever was causing AIDS might be transmissible by blood and blood products.
What follows is not intended as a comprehensive account; for that the Report should be read in full. Set out below are some of the key failings.
Infections, leading to deaths, illness and suffering were caused needlessly to people with bleeding disorders by:
• Failures in the licensing regime – in particular (but not only) by allowing the importation and distribution from 1973 of blood products (Factor 8 concentrates) made in the US or Austria which carried a high risk of causing hepatitis, and were understood to be less safe than current domestic treatments for bleeding disorders.
• A failure to ensure a sufficient supply of Factor 8 concentrates from the plasma of UK donors to meet reasonable foreseeable demand without the need to import any products from abroad (ie failure to achieve “self-sufficiency”). In part this arose from the inept, fragmented system by which the blood services of England and Wales operated; and in larger part because (a) the fractionation facilities in England (“BPL”) were in great need of redevelopment, but this was badly delayed; and (b) new fractionation facilities in Scotland (“PFC”) which had been designed and funded to produce blood products for the North of England as well as Scotland were not utilised for that purpose.
• Increasing the size of the pools used to manufacture factor concentrates (both 8 and 9) in the UK, although it was well known that this would markedly increase the risks of viral transmission.
• Whilst presiding over this increase, failing to encourage and finance research into methods of viral inactivation of factor concentrates (both 8 and 9).
By failing to do so, failing to achieve the total or at least partial viral inactivation of hepatitis viruses (in domestic production) by around 1980/1981 which would probably have resulted from such research if it had been pursued earlier (no new technology was needed). Viral inactivation could have prevented many infections (hepatitis and later HIV) and deaths.
• Also, by failing to do so, failing to provide factor concentrates which would with rare exceptions have been free of active HIV virus.
• Failing to ensure sufficiently careful and rigorous donor selection and screening (and allowing continued collection of blood from prisons).
• Adopting an attitude of denial towards the risks of treatment with factor concentrates.
• Treating people with ever increasing volumes of concentrates despite the increased risks of viral transmission.
• Failing to respond to serious risks of infection by making adjustments to treatment regimes to make them safer: such adjustments might have included greater use of cryoprecipitate (and, on a temporary basis, fresh frozen plasma) and of DDAVP, taking a more conservative approach to treatment, reducing the amount of home treatment, avoiding prophylactic treatment, adopting batch dedication policies, and deferring elective or non-urgent surgery.
• Treating children at Treloar’s with multiple, riskier, commercial concentrates, prophylactically and as objects for research.
• Treating children unnecessarily with concentrates (especially commercial ones) rather than choosing safer treatments.
• Failing to provide advice, guidance and information to clinicians to ensure that safer treatment practices were adopted.
• Adopting the wrong approach by looking for conclusive proof of what was the cause of AIDS rather than asking if there was a real risk that blood might transmit it.
• Falsely reassuring the public and patients – that blood did not carry AIDS; that the risk of AIDS for people with bleeding disorders was small; and that non-A non-B Hepatitis (Hepatitis C) was relatively mild and inconsequential.
• Taking a decision in July 1983 not to suspend the continued importation of commercially produced blood products.
• Having made that decision, failing to keep it under review.
• Failing to tell people of the risks of treatment and of available alternative treatments, thus treating them without their informed consent.
Conducting research on people without, in many cases, telling them (or in the case of children, their parents) beforehand, or informing them of the risks and whether the research would enhance their treatment or primarily benefit others, and without obtaining properly informed consent.
• In some cases, failing to tell people that they were infected and thereby denying them the opportunity to control the progression of their own illness more effectively and to prevent the spread of infection to others close to them.
Infections, leading to deaths, illness and suffering were caused needlessly to people who received blood transfusions by:
• Failing to ensure sufficiently careful and rigorous donor selection and screening (and allowing continued collection of blood from prisons).
• Failing to take all reasonable steps to deter high risk donors, in particular by delay in the production of AIDS donor leaflets and failing to ensure their effective distribution and wording.
• Missing the opportunity to screen out some high risk donors by surrogate testing as a response to the risk of HIV transmission.
• Failing to introduce surrogate testing for anti-HBC and ALT when it could and should reasonably have been introduced to reduce transmission of non – A non – B Hepatitis (Hepatitis C).
• Delaying universal screening of blood donations for the presence of HTLV-3 (HIV) despite it being urgent (it was a public emergency) to begin this.
• Delaying universal screening of blood donations for the presence of Hepatitis C.
• In particular, delaying screening for HIV and or Hepatitis C by unreasonably requiring, or if required delaying, an evaluation of different tests (which would have been reasonably effective) to see which was best (making the best the enemy of the merely good).
• Failing to warn patients of the risks of transfusion at least in situations where they reasonably had a choice.
• Giving too many transfusions when they were not clinically needed, or when less would have sufficed, or over-riding a patient’s wish not to be transfused.
• Failing to make maximum use of alternatives to transfusion.
• Failing to take sufficient and timely steps to ensure the better use of blood by hospitals and clinicians.
• Failures of record keeping to enable each unit of blood to be traced from donation to use in treatment.
Failing to carry out any lookback at the time universal screening of donations for Hepatitis C was introduced.
• Delaying telling patients they had Hepatitis C, or should be tested for it, thereby preventing the individual from controlling its worst effects, seeking timely treatment, and limiting the spread to others.
So far as both people with bleeding disorders and people receiving transfusions were concerned, clinicians and the health service in particular failed them by:
• Being complacent about the risks of non-A non-B Hepatitis (Hepatitis C) and being slow to respond to the risks of AIDS.
• Being too slow to establish an expert advisory committee on AIDS and too slow to establish an overarching body with responsibility for blood safety.
• Failing to tell people of the risks of treatment or transfusions, and failing to seek their consent on a properly informed basis.
• Failing to offer people reasonable alternatives to treatment or transfusions.
• In far too many cases, using insensitive and inappropriate means to tell people of their infections.
• Testing samples (which in most cases patients did not know were to be retained for the purpose) without their knowledge or consent.
• Delaying informing people of their infections by weeks, months and sometimes years.
• Too often compromising patient confidentiality and adding to stigma by prominent indications that these patients were a high risk to others.
• Failures of record-keeping, such that many people’s medical records have been destroyed or lost or are materially incomplete.
So far as all the people who were infected and affected were (and are) concerned, the harms done to them were compounded by:
• Repeated and ongoing failures to acknowledge that they should not have been infected.
• The absence of any meaningful apology and redress.
• Repeated use of inaccurate, misleading and defensive lines to take which cruelly told people that they had received the best treatment available.
A lack of openness, transparency and candour, shown by the NHS and government, such that the truth has been hidden for decades.
• Deliberate destruction of some documents and the loss of others.
• Failing to provide psychological support and counselling to people who had been infected and their families.
• Difficulties and delays in accessing appropriate specialist treatment and monitoring for Hepatitis C.
• Failures of palliative care for those dying in consequence of infection with HIV or hepatitis.
• Refusal to provide compensation (on the ground there had been no fault).
• Long delays in agreeing to provide even ex gratia financial support.
• Establishing ex gratia payment schemes which were underfunded and did not function in the best interests of those infected and affected.
• Failing to reform those ex gratia schemes promptly and failing to ensure that the national schemes which replaced them offered parity of support across the UK.
• Responding to calls for a public inquiry by producing flawed, incomplete and unfair internal reports.
• Failing, until 2017, to decide to establish a public inquiry.
• Failing as yet to respond to many of the recommendations of Sir Robert Francis KC, and those of this Inquiry in its second interim report.
It will be astonishing to anyone who reads this Report that these events could have happened in the UK. It may also be surprising that the questions why so many deaths and infections occurred have not had answers before now. Those answers cannot be as complete as they might have been thirty years ago, and I acknowledge that despite the vast number of pages of documents which the Inquiry has examined, some questions must remain unanswered. Any errors, any omissions, any shortcomings are mine alone.
I have no doubt however that, despite the difficulties of time and scale, the conclusion that wrongs were done on individual, collective and systemic levels is fully justified by the pages that follow; that a level of suffering which it is difficult to comprehend, still less understand, has been caused to so many, and that this harm has, for those who survived long enough to face it and for those who, infected and affected, are now able to read this, been compounded by the reaction of the government, NHS bodies, other public bodies, the medical professions and others as described in the Report."
You can read the full report: www.gov.uk/official-document The victims of this scandal deserve and have long awaited full compensation.

On Wednesday 15 May 2024, the House of Commons considered the Criminal Justice Bill. The Bill contains various measures which the Government says will protect the public, give the police the powers they need to cut crime and anti-social behaviour, improve public confidence in the police, introduce tougher sentencing for sexual and violent criminals and strengthen the supervision of offenders on release from prison. I support this Bill. There are many measures within in it that I have supported calls for, such as the introduction of corporate criminal liability, stronger sentences on sexual offences, and the crack down on antisocial behaviour by going after drug dealers with stronger closure orders. However, I am concerned at how long it has taken to bring forward such measures. I also consider that the Bill does not go far enough to deal with the deep problems the criminal justice system now faces after a decade of decline. I supported a new clause in the Bill that would have introduced a ban on ninja swords, dangerous weapons which have been used to kill teenagers on Britain’ streets. Unfortunately, this measure was voted down by Government MPs. I was also disappointed that a new clause that would have amended parts of the Sexual Offences Act 2003 to replace the term “prostitution” with “sexual exploitation”, in order to stop victims of adult sexual exploitation from being wrongly identified as consensually engaging in sex work, was also defeated.
I welcome though that the Government has made concessions and listened to concerns raised by MPs about the Bill in other areas. I support, for example, new clauses that were added to the Bill to make it an offence to create a sexually explicit deep fake image of an adult without their consent; to make it an aggravating factor if an offence of manslaughter involves sexual conduct; and to make ‘cuckooing’ – where people take over another person’s home for the purpose of criminal activity by coercion, threats or abuse of a position of vulnerability – a specific offence. I am also pleased that the Bill now provides for an automatic suspension of parental responsibility in cases where a father is convicted of child rape, although I am concerned that this does not extend to other serious sex offences against children. The Bill was also amended to create a new offence of causing death or serious injury by dangerous, careless or inconsiderate cycling and to strengthen sentences for criminals who sexually abuse the dead.
The House of Commons will consider further amendments to the Bill at a later date.
I voted Aye for both stages and these are the results:
Criminal Justice Bill Report Stage: New Clause 44 - Ayes: 167 Noes: 275
Criminal Justice Bill Report Stage: New Clause 59 - Ayes: 171 Noes: 272

It was good to meet the team from REACT who are involved in supporting Government organisation in times of national pandemic. React played a part in Walsall in helping to administer the vaccine. The volunteers are former service people who are putting their skills to use to support society. I met Jonny and Cheese. you can find out more here: Website: https://www.re-act.org.uk/

On 12 May 2024 I appeared on BBC Sunday Politics from the Midlands. The other guest was Daniel Kawczynski MP.
You can view the BBC Sunday Politics show on the website
Videos
Covid Memorial Wall
20mph Speed Limits
RAF Centenary Flypast